About hormone therapy (HT) (also known as hormone replacement therapy – HRT)
For more frequently asked questions about hormone therapy issues go to:
Answers to Questions about Hormone Therapy and Coronary Heart Disease
What is menopause and when does it start?
Menopause is literally the very last period of a woman’s reproductive life. It is said to occur when a woman has not menstruated naturally for 12 consecutive months. Menstruation ceases because the ovaries no longer produce ova (eggs) and the monthly reproductive cycles stop. The average age for menopause is 51 years with the normal range being from 45 to 60 years.
What are the common menopausal symptoms?
The most common menopausal symptoms are hot flushes, night sweats and vaginal dryness. Other symptoms that can occur include anxiety, poor memory, poor concentration, insomnia, fatigue, palpitations, decreased libido, muscle pains, crawling skin and urinary problems. Mild depression or other mood changes may occur during the time of physical and erratic hormonal changes (i.e. in the perimenopause or time before the periods stop) but severe depression is not caused by menopause nor is it more frequent at menopause. Women who have had a history of depression, before the menopause, or who have a history of PMS (premenstrual syndrome), may be more sensitive to the changes taking place.
Do all women experience symptoms at menopause?
No, between 10 and 20 per cent of women have no symptoms, 60 per cent experience mild to moderate symptoms and 10 to 20 per cent experience severe symptoms. In some women physical symptoms, like night sweats, are predominant while other women may have few or no physical symptoms but experience significant psychological symptoms. Women who have significant psychological problems such as depression or severe PMS may need specific treatment or counselling.
Is a woman menopausal if her periods are regular but she is feeling down and has difficulty remembering things?
It is possible for a woman, usually in her forties or early fifties, to have menopausal symptoms even if she still has a regular period. Some women experience mood symptoms, like anxiety and depression, for several months to several years before periods actually cease. This is due to gradual changes in the ovaries and fluctuating oestrogen levels. This transition time, which averages four to six years before the menopause, is called the perimenopause.
Is depression a symptom of menopause?
Depression is not a symptom of menopause. Although some of the physical changes may affect wellbeing, most women cope. In Western societies we are concerned about remaining young which often leads to us having negative attitudes about reaching menopause. In contrast, other societies, such as in many Asian countries, reaching menopause and growing older elevates women to a higher status within a community. Menopause may act as a trigger in women who have a history of depression.
Should hormone levels be checked?
Hormone levels are of relatively little value. They may help to gauge the onset of menopause when a woman has had a hysterectomy or if menopause is suspected in women under the age of 40; however hormone levels change rapidly from one day to another in the perimenopause and are not helpful in diagnosing menopause. Having symptoms is a better guide.
Is a woman likely to have an early menopause if she has had a hysterectomy but still has her ovaries?
Between 10 and 20 per cent of women who have had a hysterectomy have earlier menopause, between one to four years earlier than their expected menopause.
What are the best ways of coping with menopausal symptoms?
There are many ways of coping, though it often depends on the severity of the symptoms. Many women cope with mild symptoms without any medication. Regular exercise often helps because this promotes wellbeing, enhances relaxation and sleep, and may reduce menopausal symptoms.
Good eating habits with foods rich in phytoestrogens such as soy products or linseed may be beneficial. Women with mild to moderate symptoms may prefer to take herbal or plant hormone therapies, which should be either monitored or prescribed by a qualified naturopath or herbalist with an interest in women’s health. Women with more severe symptoms usually find hormone therapy (HT) the most beneficial.
What is HT or HRT?
This treatment is used to restore the important female hormones that the ovaries stop producing after menopause. Oestrogen is the main hormone prescribed to relieve menopausal symptoms. If a woman still has her uterus she must also take progesterone-like hormone (progestagen).
Progesterone protects the uterus lining from over-stimulation by oestrogen, which in the long-term may lead to uterine cancer. Women who have had a hysterectomy do not need progestagen. Women experiencing loss of libido (sex drive), lack of energy and on-going fatigue, even when taking oestrogen therapy, sometimes benefit from low-dose testosterone replacement. However, it is important to discuss with the individual woman psychological and relationship issues as well.
There are different ways of taking HT and different combinations of the three hormones; oestrogen, progesterone and testosterone. Usually tablets are orally prescribed but there are also patches, a gel, implants and vaginal preparations such as creams or pessaries.
The patch is applied to the skin on the lower body once or twice weekly, the gel is applied daily and the implant (hormone pellet) is inserted under local anaesthetic beneath the skin and usually lasts four to six months. In all the non-oral routes the hormones are absorbed directly into the blood stream whereas with tablets they are absorbed through the intestine first.
What are the effects of HT?
Oestrogen prevents postmenopausal bone loss of calcium and protects against osteoporosis, and oestrogen reduces the risk of colon or bowel cancer. The WHI study originally published in 2002, showed no increase in risk of heart disease and stroke in the 50-59 age group, and a small increase in risk in the 60-79 year old group. There was a small increase in risk of breast cancer after 4-5 years of HT.
However, in a younger woman taking HT for menopausal symptoms the risks are likely to be very small. All women should discuss their individual circumstances with their doctor.
What are the common side effects of HT?
The most common undesirable effects from oestrogen therapy are breast soreness and nausea. These symptoms generally improve over time or by altering the dose or treatment method. The progestagen may cause side effects including bloating, depression and mood swings which are similar symptoms to premenstrual syndrome.
Who should not take HT?
Most women are able to take HT. However, in some groups of women, therapy is not advisable and alternatives should be used where possible. These include women who have had cancer of the breast or uterus, a history of thrombosis (blood clots in veins or lung), severe liver disease or undiagnosed vaginal bleeding, heart disease or stroke.
Does HT cause weight gain?
Studies have shown that men and women tend to gain weight as they age. Genetic, family, environmental, lifestyle and some hormonal factors (like an underactive thyroid gland) can contribute to weight gain. With ageing, the base metabolic rate tends to decline and weight increases if the energy intake from food and beverages is more than the energy used in daily activities and exercise.
Gaining weight specifically from HT is uncommon. This may occur temporarily when starting HT, but it is usually from fluid retention and is related to the body readjusting to changing hormone levels.
Many women, but most commonly those not on HT, notice that they lose their waistline. This is due to a 10 per cent redistribution of body fat from the hips and thighs to the abdominal (stomach) region, and is related to hormonal changes at menopause as well as ageing. Regular exercise is particularly beneficial when combined with a well-balanced diet.
Having foods that are low in fat and high in calcium help reduce the risk of heart disease and osteoporosis. Phytoestrogens from soy products, seeds, legumes, fruits and vegetables may also decrease the risk of these diseases, help treat mild menopausal symptoms and prevent some cancers. .
Does HT cause breast cancer?
HT does not cause breast cancer, but long-term HT is associated with a slight increase in the risk of developing breast cancer. There has been much research into this issue with some studies indicating small risk and others indicating no risk. The report from the American Women’s Health Initiative (July 2002) indicated that there is a small increase in breast cancer risk in women taking combined continuous oral hormone therapy. To date this study has not indicated any increase in risk for women taking oestrogen alone after they have had a hysterectomy. The increase in risk translates to eight extra cases (41 women versus 33) for every 10,000 women treated for one year.
Any decision about HT is an individual one and should be made after each woman is informed about her individual risks, benefits, needs and concerns in consultation with her prescribing health practitioner.
How long should a woman stay on HT?
For the treatment of symptoms, women can stay on HT for two to five years. After five years, the need to continue should be reviewed annually and the reason for taking HT reassessed e.g. severe symptoms. In 10 per cent of women, menopausal symptoms may continue for longer than 10 years and these women may require HT for symptom control for longer periods. Current guidelines recommend that women who take HT for menopausal symptoms take the lowest effective dose for the shortest time period to alleviate symptoms.
For established osteoporosis or bone protection, less than five years use is also currently advocated and long-term use is considered a second-line choice.
Do menopausal women have decreased sexual interest and activity?
Sexual interest or libido depends on many factors, not just hormonal levels. Stresses of daily life, poor physical health, medications, relationship conflict or psychological problems can affect sexual wellbeing. Most studies on sexuality in menopausal women indicate wide variations. All factors need to be assessed.
Lower oestrogen levels can result in vaginal dryness and discomfort during intercourse but this problem can be treated with appropriate lubrication or oestrogen therapy.
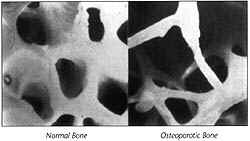
What is osteoporosis?
Osteoporosis occurs when bones lose their strength and density, and become fragile and fracture (break) more easily due to a loss of calcium and bone framework. This disease particularly affects women in their middle and later years and is painless until a fracture occurs. It is quite different from osteoarthritis which affects joint surfaces and is painful.
Should all women have a bone density measurement?
No, each woman should be assessed by her doctor about the risk of developing osteoporosis and then be referred for a bone density measurement if necessary.
What are the risk factors for osteoporosis?
The most reliable risk factors are a family history of osteoporosis, early menopause, (occurring before the age of 40), a thin, small body, and being Caucasian or Asian. Other equally relevant factors are smoking, a high intake of alcohol and caffeine, certain medications such as long-term cortisone, low vitamin D levels and diseases like an overactive thyroid or anorexia nervosa.
What tests are available to assess the risk of developing osteoporosis?
Several tests are available for measuring bone density, the most common and reliable being x-ray bone density (DEXA). The DEXA method measures bone density at the sites of greatest concern – the hip and the spine – using low dosage radiation. One in three women reaching the age of 60 years will suffer a hip fracture.
However the results of DEXA alone do not adequately predict a woman’s risk of fracture. To predict osteoporosis fracture risk, the risk factors discussed in Question 19 should also be considered..
How does taking HT prevent osteoporosis?
HT prevents the accelerated bone breakdown that occurs during the early post-menopausal years, therefore reducing the likelihood of fractures. However, because of the small but significant risks of long-term HT use over the age of 50, other alternatives should be considered. These include exercise, diet, calcium, adequate vitamin D levels and other medications.
Are calcium supplements necessary?
Post-menopausal women are recommended to have 1200-1500mg of dietary calcium each day (three glasses of milk or equivalent). Women who have difficulty consuming this amount should consider a calcium supplement at night. Although calcium does not prevent bone loss, it is important in the overall prevention of osteoporosis when combined with exercise, oestrogen and other therapies. Recently, studies in older women suggest one gram of calcium supplement (more than one tablet daily) may increase the risk of heart disease, but further research is needed.
What natural therapies can I take?
Women at midlife may decide to try a variety of natural or complementary therapies to manage symptoms or create more comfort for themselves. For more information about natural or complementary therapies go to Other Therapies
What can I use to make intercourse less painful and dry?
Oestrogen loss at midlife causes much of the discomfort (e.g. vaginal dryness or painful intercourse) that can occur during penetrative sex. Water based lubricants (e.g. Lubofax, Sylk, KY Jelly, Replens) may help to relieve discomfort during sex. Oestrogen vaginal cream, tablets or pessaries may improve vaginal secretions and relieve symptoms.
Does HT protect against heart disease?
For information about hormone therapy and heart disease please go to HT and Heart Disease Q&As
How long will my menopause symptoms last?
Menopause symptoms occur in 80 per cent of women. In 20 per cent of women symptoms are severe and in 60 per cent symptoms are mild to moderate in severity. In 75 per cent of women symptoms will last up to five years, and in 10 per cent symptoms will last longer than 10 years.
How early can a woman reach menopause?
The average age for menopause is 51 years with the normal range being from 45 to 60 years. Menopause before the age of 40 is termed ‘premature menopause’ and menopause between the ages of 40 and 45 is termed ‘early menopause’. It may occur spontaneously as a result of early failure of the ovaries; be caused surgically when a woman has her ovaries removed; or be caused chemically by chemotherapy for cancer.
For more information go to Early Menopause
Can exercise stop osteoporosis?
In the adult years exercise is beneficial for bone health even though peak bone mass has already been achieved. Exercise is beneficial in a number of ways as it increases muscle strength, assists with posture and balance and thereby reduces the likelihood of falls.
For more information go to Bonehealth
What should I know about testosterone?
Until menopause, a woman produces three different natural female hormones: oestrogen, progesterone, and testosterone. Oestrogen and progesterone are produced in the ovaries during a woman’s reproductive life. Testosterone is produced by the adrenal glands and the ovaries and is useful for muscle strength, wellbeing and sexual functioning. In women, testosterone levels start decreasing from age 35 but continues to be produced throughout life. Testosterone therapy may be helpful in some women.
For more information go to:
Testosterone
Testosterone for Women – written for health professionals.
What should I know about libido?
Libido is about your sexual interest and desire. Menopause is a natural event in a woman’s life cycle and loss of libido (reduced desire and sexual experiences that are no longer satisfying or pleasurable) may be one of the symptoms experienced around this time.
For more information see Libido
What should I know about ‘bio-identicals’ hormones?
For a discussion about ‘bio-identicals’ or ‘bio-identical hormones’ please go to Bio-identical Hormones
What is the best way to stop using HT?
There is no good research evidence on this, but it is generally accepted that the best way to stop HT is to reduce it gradually over a few weeks or months (unless there is a good health reason for stopping suddenly on your doctor’s advice). Hot flushes often return after stopping HT, sometimes immediately, sometimes after a few months, and weaning off gradually is the best way to adjust to and manage this.
Talk with your doctor before stopping or reducing your HT.
Will the symptoms return if I stop HT?
We do not know if hot flushes get better, worse or stay the same when HT is stopped; it depends on the length of time each individual woman will have her symptoms. There is no way at present to determine this.
Some women move to a lower dose after a while, and find that this is satisfactory to control symptoms. Later you may reduce the dose further by taking tablets every second or third day, or cutting your patch in half (this can only be done with a matrix patch). If symptoms return, you can go back up to a higher dose of HT and try reducing it again later. Eventually your symptoms will lessen – how long this takes varies from woman to woman.
Do the HT risks continue when I stop using it?
We do not know. The evidence to date is not clear on this except for breast cancer where evidence confirms that the risk returns to that of non users within five years of stopping HT.
Top Steroid Products Sales
Masteron 500 (5ml)
|
Clenbutaxyl
|
Clenbutaxyl
|
 by Gen-Shi Laboratories")

